
WV GOP Plan for Opioid Crisis: Don’t Do Drugs. If You Do, Die Quickly.
WV GOP Plan for Opioid Crisis: Don’t Do Drugs. If You Do, Die Quickly.
The opioid crisis is a community crisis; we can't address one without the other.


Needles have had a way of putting West Virginia in the national news lately.
On the one hand, West Virginia has set a gold-standard for vaccine distribution.
On the other hand, the CDC recently declared an HIV outbreak in Kanawha County (where the capitol is located) “the most concerning in the United States.”
As the Associated Press reports:
The number of HIV cases tied to drug use in Kanawha has been increasing since 2018, when there were two. In 2019, there were 15 and at least 35 were reported last year, according to Shannon McBee, the top epidemiologist with the West Virginia Department of Health and Human Resources. In comparison, New York City recorded 36 HIV cases tied to intravenous drug use in 2019, according to the CDC.
It has been almost 20 years since opiates first gripped the region. By now, the opiate crisis has reached across every living generation, every class, every race. There’s no reason to pretend that there is anyone in America who has not been touched by it in some form or another.
But as the CDC notes, the crisis in West Virginia is particularly alarming.
The CDC’s comments came in the midst of a debate about a ‘controversial’ syringe service program in Charleston, and as the AP reports, CDC officials were clear that
“officials need to act quickly to slow the spread of HIV and hepatitis, said Demetre Daskalakis, head of the CDC’s HIV/AIDS prevention program. A syringe service program could help, but there's also a need for community education, he said.
There needs to be widespread community buy-in for progress to be made, [Epidemiologist Shannon] McBee said.”
So of course, our so-called ‘conservative’ legislature is looking to exert control over local needle exchange programs.
Charleston’s WCHS reported on Thursday, March 11:
“Such programs are designed to help contain the spread of infectious diseases that sometimes linger in used syringes. The bill would require licenses for syringe collection and distribution programs. Operators would have to offer an array of health outreach services, including overdose prevention education and substance abuse treatment program referrals. Opponents say the bill's stringent measures would force existing syringe exchange programs to close.”
This regulation isn’t about making them better. This regulation derives from conservative Republicans’ preference for a tough “law and order” approach to drugs and addiction, one which has the chief aim of eliminating the supply of drugs in an area. It is one of the places that anti-regulation and small government conservatives are in favor of regulation and government interference.
And when they address the demand side of the equation, they only focus punishing drug users.
It is a prohibition approach to addiction, one that failed so thoroughly with alcohol that the U.S. passed an amendment to repeal the amendment that banned alcohol to begin with.
These approaches have failed for 90 years, and they continue to fail.
All prohibition does is create a very lucrative black market for drugs, and in the case of needles, restricting access to clean needles just encourages users to re-use and share needles, which is one of the main ways that HIV is transmitted.
These regulations also force individuals who are in the throes of addiction to the margins of society, at exactly the moment that they most need community and social support. Heavily criminalizing drug use does not encourage a drug user to seek help. If it did, then the Nixon/Reagan War on Drugs the Clinton-era minimum sentencing laws of the 90s should have eliminated drug use in the United States by now.
Prohibition fails for one simple reason. It addresses drug use as an originating cause of social harm and social breakdown, rather than as an effect of social harm and social breakdown.
In the conservative worldview the cause-and-effect chain looks something like this: drug use leads to unemployment, which leads to family neglect and homelessness; homelessness leads to panhandling and property crimes; these things make communities unsafe, which leads to lower property values, which leads to drug houses, which attracts drug dealers and prostitution, and thus Parkersburg becomes New Gomorrah and Charleston becomes New Sodom.
With this logic it is easy to see how ‘just one toke’ could ultimately destroy the moral fiber of our communities, why there is so much emphasis on the individual’s responsibility to say no to drugs, and why many people hold contempt for addicts rather than compassion. Under this logic, it is easy to conclude that the only solution is to purge addicts from communities: just throw them in jail and ban panhandling and crack down on homelessness; force them to move on to another community.
But that logic does not provide adequate explanation of why there are geographic hotspots for the opioid crisis. When one looks at the relationships between poverty rates and opioid sales, and poverty rates and opioid usage, the correlation is stark.
One 2016 report from Health and Human Services explored exactly that. The keys on these images are small, but simply, purple areas are why poverty is high and opioid sales and use are high.
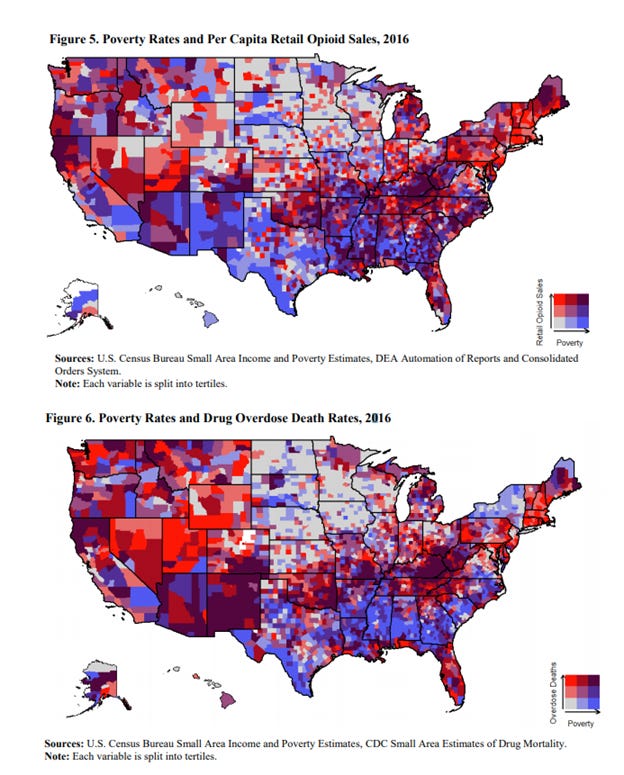
As the authors summarize,
“(1) The prevalence of drug overdose deaths and opioid prescriptions has risen unevenly across the county, with rural areas more heavily affected. Specific geographic areas, such as Appalachia, parts of the West and the Midwest, and New England, have seen higher prevalence than other areas.(2) Poverty, unemployment rates, and the employment-to-population ratio are highly correlated with the prevalence of prescription opioids and with substance use measures. On average, counties with worse economic prospects are more likely to have higher rates of opioid prescriptions, opioid-related hospitalizations, and drug overdose deaths.”
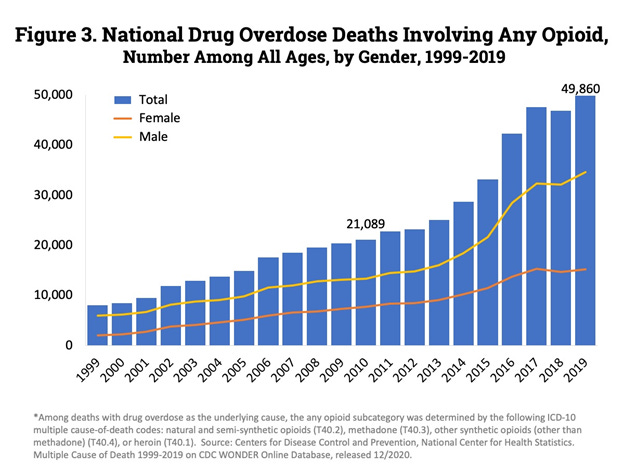
Conservatives should find these explanations at least somewhat appealing, because I think when one correlates the geography with the timeline, and the gender disparity in overdose deaths, the North American Free Trade Agreement comes out as a driver.
If we assume NAFTA accelerated job losses in the Rust Belt (it did), and that job losses cause depression and despair (it can), then the increase in overdose deaths after 1999 starts correlating neatly with accelerated job losses from NAFTA.
If you have been working through back pain for 30 years and your job and your pension suddenly disappears, what else to do but manage the pain you’ve been left with? If you are a young man or woman with a high school degree or less, what job prospects are left for you beyond clerking at a Dollar General, a Sheetz or a liquor store? Those wages will never afford a home or a real vacation, but they might afford a few hours of numbness; and when the option is a reality of despair or chasing a high of numbness, it is understandable why desperate people choose numbness.
That’s a partial explanation for the geographic concentration, but far from a complete picture of who uses opiates.
There are plenty of college educated people who see a bleak future and are saddled with so much debt that they are also left constantly reaching for the American Dream, which now seems like a gold ring on the merry-go-round—even if it can be touched, it can never be held.
There are plenty of veterans (about 1 out of every 10 West Virginians) who have returned from our foreign wars often disillusioned and unable to adjust to civilian life (see Sebastian Junger’s work, Tribe: On Homecoming and Belonging for more on that), and they treat their physical injuries and their trauma with numbness. Again, understandable.
These are some of the places where addiction begins—it is not a individual’s moral failing; it is a society’s moral failing.
Economists Angus Keaton and Anne Case have made a convincing case that despair is a driver of suicide, overdose, and alcoholism, and researchers are now looking to define despair clinically so that it can be treated appropriately as an epidemiological driver.
In a broad social sense, I think the phenomenon is that people are more likely to become addicted to drugs when they intuitively feel like the social contract has been broken and that life provides neither opportunity nor safety.
The HHS report points to poverty, Deaton & Case point to despair, and there is a substantial body of research showing that inequality is a driver of pretty much any social harm you can think of. The Equality Trust out of the United Kingdom has pulled much of this research together, but the summary is: less equal societies have more social harms.
The Equality Trust is an incredible reservoir of research on this topic, and I encourage readers to check out the webpage, but here are the summaries of the broad impact categories.
“Crime: Inequality increases property crime and violent crime. A reduction of inequality from Spanish levels to Canadian levels would lead to a 20% reduction in homicides and a 23% reduction in robberies.
Health: Living in an unequal society causes stress and status anxiety, which may damage your health. In more equal societies people live longer, are less likely to be mentally ill or obese and there are lower rates of infant mortality.
Trust, Participation, Attitudes and Happiness: Inequality affects how you see those around you and your level of happiness. People in less equal societies are less likely to trust each other, less likely to engage in social or civic participation, and less likely to say they're happy.”
Putting stringent regulations on needle exchanges, criminalizing poverty, shaming and arresting users, breaking up families, and treating addiction as a moral failing: these do nothing to address poverty, despair, or inequality.
These punitive law and order approaches are equivalent to saying to drug users “your addiction has cause social death, and we’d prefer you to die or leave before you hurt our community more.” (As Alan Grayson once summarized the GOP plan for national healthcare: ‘don’t get sick. If you do, die quickly.”)
If we as a state, and as a country, want to save lives and reduce harms from addiction, we need to address the interconnected roots of poverty, despair, and inequality.
We need to make the American Dream something that is not just reachable like a merry-go-round gold ring that just slips away, but something that is attainable.
We need to create opportunity in the state; we need to raise wages so that homeownership is an attainable goal for average West Virginians; we need to invest in our education and vocational programs so that our young people can get good jobs in the trades or go to college if that is their drive. We need to create opportunity beyond extractive industries and cashiers for out-of-state corporations.
We also need to provide shelter to the homeless—not try to drive them out. How can someone get a job without an address, a phone, or an email? And how does someone afford a place to live without a job?
We need to invest in mental health and counseling services for adults and children alike, because our despair is deep and intergenerational.
We need to invest in community services and invite back into our communities those individuals who have been marginalized by addiction, and in doing so curb our future intergenerational despair by rebuilding our communities in the present.
Our opioid crisis is also a community crisis, and we cannot truly address one without addressing the other.